Managed-care companies overstate
the number of physicians available
to treat the state’s sickest patients
By J. David McSwane and Andrew Chavez | Staff Writers
Photos and video by Tom Fox | Senior Staff Photographer
Published June 4, 2018
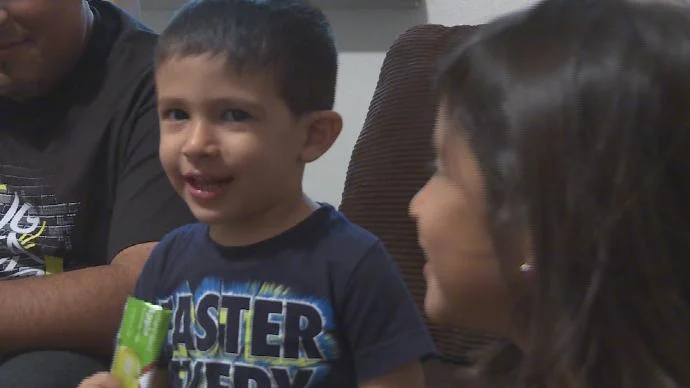
Marta Whitworth’s 12-year-old foster son needed antipsychotic drugs to tame the violent outbursts that doctors attributed to fetal alcohol syndrome.
When the boy’s psychiatrist retired last summer, Whitworth looked for a replacement within driving distance of her home in Kosse, a small town about 45 miles southeast of Waco. Because the child is in the Texas foster-care program, a company paid by the state must handle all of his health care.
A Superior HealthPlan “service coordinator” gave Whitworth a list of about a dozen psychiatrists the boy could go to — the only ones he could go to. But when she called, not one would give him an appointment within six months, she says. Several said they don’t accept Superior patients.
Years of poor state oversight have allowed companies to skimp on essential care for sick kids and disabled adults. Catch up.
Off his drugs for weeks, the boy threatened a sibling with a knife, shouting and repeating phrases over and over. Then he had a mental breakdown at school, Whitworth says. He screamed, threw chairs and ended up in a psych ward.
“He was hospitalized for four days,” says Whitworth, a school bus driver. “We could have avoided it if a doctor would have seen him.”
Her family’s experience is a symptom of a much larger problem with what’s known as Medicaid managed care, The Dallas Morning News found.
The companies Texas hires to care for its sickest citizens — foster children, chronically ailing kids, elderly and disabled adults — have been vastly overstating the number of doctors and specialists available to treat them.
In their published networks, the companies include many physicians who aren’t taking new patients, don’t accept government-funded health plans, or aren’t even treating Texans anymore. And state health officials know it.
In February, we tried to contact every psychiatrist Superior listed as available to help foster kids.
We called the main phone number in the company’s online directory for each doctor and asked the staff if they could schedule a new-patient appointment for a foster child. Only 9 percent could.
In the end, we found just 34 psychiatrists across the state who could take a foster child as a new patient. There are more than 30,000 foster kids — more than a third of whom need counseling, according to state data.
In Dallas, just seven out of 119 psychiatry offices we called within an hour’s drive of downtown said they were actually accepting new patients. Not one was within the city limits.
Marta Whitworth struggled to find a psychiatrist for her foster son (not pictured) who has severe behavioral issues. Superior HealthPlan gave her a list of about a dozen doctors; none could get her son in within six months.
“Some of these networks are really, truly a sham,” says Dr. John Burruss, chief executive of Metrocare Services, a nonprofit mental health clinic in Dallas.
Superior disputed our findings.
“We do not believe that the method you followed for selecting providers on our website is representative of the approach our members would follow,” said Jane Hardey of Marathon Strategies, a New York public relations firm representing Superior.
The state has done little to verify the accuracy of managed-care companies’ network directories, and when it has found problems, it has often given the companies a pass.
Nor have state officials addressed a primary reason networks are so limited: low pay for doctors and their staffs.
Meanwhile, many children can’t get hearing aids, or allergy treatments, or drugs to treat depression and mood disorders.
The state says it is cracking down on companies that don’t have enough doctors. It has told at least 16 health care groups, including Superior, to submit plans for how they’re going to fix holes in their networks, said Carrie Williams, a spokeswoman for the state health commission.
“Having an adequate network of providers is a longstanding challenge for Texas that predates managed care,” Williams said in a statement.
After more than 450 phone calls, we found only 34 psychiatrists who could see foster children for routine treatment.
Failed networks
Federal regulators require states that hand off Medicaid to private companies to hire outside researchers to study, among other things, how hard it is for patients to get the care they need. Since 2002, Texas has used a team at the University of Florida to do its quality assessments.
A managed care program for people who have disabilities or are age 65 or older. Many of these patients need nursing-facility-level care in their homes such as hospital beds and breathing machines.
In 2016, the group began conducting “secret shopper” calls, in which academics pose as patients trying to arrange doctors appointments. When the undercover callers tried to get mental health care through the state's program for the elderly and disabled, only about 1 in 5 accepted the plan and were able to schedule an appointment, according to public documents The News obtained through open-records requests.
About 27 percent of the doctors they called said they didn’t take Medicaid. The next year, researchers found that trend had gotten worse — 38 percent of doctors said they weren’t taking the government program.
But the state gave several health care companies passing grades for appointment availability. How? It just didn’t count all the doctors whose phone numbers didn’t work or who didn’t accept Medicaid.
Without those doctors in the sample, it appeared that more than 88 percent of doctors listed in company networks could see a patient within days or weeks. But in reality, only 14 percent of doctors were taking appointments.
Specialists are most likely to care for extremely sick Texans. For a decade, health officials collected data tracking how many of them, including heart and lung doctors, dotted the state’s 254 counties.
But the state failed to analyze the data until late last year, when regulators found large swaths of Texas without available specialists.
The state has no idea how many Texans can’t find specialists, though. That’s because the health commission never asked researchers to do the “secret shopper” study for most specialties.
So The News did its own study. We called a random sample of the specialist providers listed in networks for three managed-care companies: Superior, Amerigroup and United Healthcare. We made almost 300 calls and tested six key specialities.
Of the offices we reached, 2 out of 5 of them said they either didn't accept the Medicaid plan for which they were listed or the specialist was no longer at the office. That suggests 8,000 to 11,000 of the 25,000 specialist listings would lead patients to a dead end.
Those barriers can have devastating consequences.
Velma Castillo carefully gets out of her daughter's car after picking up her granddaughter from school in San Antonio. Castillo couldn’t get help from Superior HealthPlan when she needed treatment for bipolar disorder and schizophrenia.
Velma Castillo, a San Antonio woman in the health program for the disabled, couldn’t get help from Superior when she needed treatment for bipolar disorder and schizophrenia, conditions that caused her to lash out at her family and disappear for days.
“Just to get her medicine, she would go to the hospital for two weeks,” says her daughter, Sofia Reyes. “More than a hundred times.”
In May 2016, after Superior failed to help a different patient find psychiatric care in the same county where Castillo lives, state employees called 33 different offices, according to state records.
They found only one that would see the patient.
Foster children at risk
The state never conducted a secret shopper study for the network charged with taking care of the state's foster children.
So, we did.
We called all 377 psychiatrists listed in the STAR Health program, the Medicaid managed-care plan for foster kids, and asked if the doctor listed in the directory was seeing new patients. Almost 45 percent of our calls reached a wrong number, or we were told the psychiatrist was no longer at the office we phoned.
Looking for the next great investigation to read?
If you enjoy in-depth, investigative reporting such as this, please consider supporting dallasnews.com by subscribing today.
Telephone numbers were disconnected or rang in hospital emergency rooms or were answered by fax machines.
Seven psychiatrists listed at UT Southwestern Medical Center in Dallas were not affiliated with the hospital, according to a spokesman.
Some offices said they hadn’t accepted Medicaid patients in years — or they never did — including Psymed Solutions and Aesthetics, a boutique firm in Plano whose services include Botox injections and cellulite removal for adults.
Almost 14 percent of the providers we called didn’t accept Superior’s plan for foster kids; 9 percent weren’t accepting new patients.
A decade of evidence
Network problems are not a surprise to the state. As early as 2008, auditors had warned that there were “significant deficiencies” with Amerigroup’s.
In 2011, auditors looked at a tiny piece of Superior’s specialist network and found the company had only 712 specialists in Lubbock, not the 1,554 it listed, according to state records.
Just last year, state regulators found that at least a dozen children in Bexar County — the San Antonio region — couldn’t get hearing aids. Superior didn’t have a single audiologist there.
There were hearing-aid specialists in the area, but state records show they refused to work with Superior because of “low reimbursement” and “difficulties in obtaining payment,” according to emails we obtained through open-records requests.
The problem could have long-term consequences, a state employee wrote in one of the emails: “Delay in receiving timely pediatric hearing aid services can affect the children's ability to speak.”
The state pays about 20 companies and nonprofits a flat fee to care for patients. That fee, paid for with state and federal money, is on a per-person, per-month basis and varies by the severity of patients’ conditions and needs. State actuaries determine this payment based on what they think healthcare will cost, plus 1.5 to 2 percent that can end up as profit or cover unexpected costs.
Companies like Superior and Amerigroup collect a set fee per patient, a payment known as a “capitation.” They get the money whether or not the patients visit doctors. When patients do seek treatment, the companies want to pay as little for it as possible.
“These companies are looking for physicians who are willing to take a lower rate,” says Dr. Linda Villarreal, a geriatrics doctor in the border town of Edinburg who sits on the board of the Texas Medical Association.
“Therefore, their network is very, very small.
“Their process of denials is deny, deny and deny until you just can’t anymore,” she says.
In San Antonio, Dr. Armando Garza says many of the children he sees have gotten worse as they waited months for physical and speech therapy, in limbo because of what he called Superior’s “stalling game.”
“It seems like it’s to try to save money on their end,” he says. “The kids are suffering.
“I can’t see the amount of Medicaid patients that I was seeing before,” Garza says. “I had to slow down because they’re not paying anybody, and all of our time is wasted on getting approvals,” or appealing denials.
A Superior spokeswoman called accusations that the company is denying care to save money “categorically false.”
‘Strategic narrowing’
State records suggest some companies may be intentionally thinning their networks in hopes of reducing doctor visits and bolstering their profits.
In Houston, Texas Children’s Hospital has accused Amerigroup of deliberately cutting back on its pediatric network to save money. The hospital didn’t join the company’s network because the payments were too low, an executive wrote to the state.
Yet its doctors were being inundated with Amerigroup’s most fragile children as though they “had nowhere else to turn for pediatric care,” hospital representatives wrote to the state health commission last year. They also accused Amerigroup of “strategic narrowing” of its networks to save money.
Texas Children’s Hospital in Houston has accused Amerigroup of cutting back on its network of doctors to save money.
The hospital continued to see severely sick children in Amerigroup’s plan on an “out of network” basis, a hospital spokeswoman said, because Texas Children’s employed the only specialists in the region who could treat certain conditions.
Instead of cracking down on Amerigroup, records show state regulators repeatedly gave the company a pass on its poor network in the Houston region.
Amerigroup’s plan for fragile children in the Houston area netted the company more than $3,400 per child in its first 10 months — one of the highest profit margins of any plan in any part of the state. Texas Children’s, meanwhile, lost $3,000 per child.
Olga Gallardo, an Amerigroup spokeswoman, blames Texas Children’s, which she says refused to accept the company's “fair” contract terms.
Nearby, in Jefferson and Orange counties, Amerigroup is responsible for 3,000 patients, but as of late last year there wasn’t a single ear, nose and throat doctor to serve them, according to state data.
The company is working to recruit more doctors and is expanding its telemedicine offerings, Gallardo says.
“Amerigroup is committed to maintaining a robust care provider network of more than 60,000 care providers across the state to ensure our consumers have access to high quality health care,” she says.
Jack Billingsley gazes at the 1950s Mexican guitar he sometimes plays at his ranch home near Llano. He had a stroke in 2001 that blinded him in one eye and impaired his brain function. Billingsley used to have a personal attendant, but managed-care companies are cutting those services systemwide. For a year and a half, he has struggled to get help preparing meals and cleaning his home. "I feel ashamed, living like this," Billingsley says.
Uncoordinated care
One of the main reasons Texas pays $22 billion a year to managed-care companies is to improve patients’ health through case managers whose job is to help sick people and busy foster parents find doctors.
In fact, care coordination is the chief benefit cited by the managed-care industry’s lobbying group.
“Texans who need specialized care and services benefit the most from managed care, because the system ensures each family has a nurse or social worker to coordinate care and help patients navigate the maze of traditional health care services,” Jamie Dudensing, chief executive of the Texas Association of Health Plans, said in a statement.
“More than that, care coordinators work to get patients a range of services that go far beyond traditional Medicaid, including meal coordination, home modifications, housing, and transportation.”
But the companies haven’t hired enough coordinators, and those they have on staff are often referring patients to dead-ends, the state’s own research shows. A report last year by the nonpartisan Legislative Budget Board found that “most members in managed care programs receive minimal or no coordination services from their managed care organization.”
Worse, patients “with the highest needs often experience the largest gaps in access to services that should be coordinated by their managed care organization.”
For example, these coordinators serve under 20 percent of foster kids, according to several state studies, even as the state pays Superior more than $10,000 a year per child. One report blames uncoordinated case management for the fact that many foster children aren’t getting mental-health treatment.
For the quarter-of-a-million elderly and disabled people in Medicaid managed care, coordination is even worse. Year over year, more of those Texans have reported difficulty getting doctor appointments and more basic assistance.
In 2001, Jake Billingsley had a stroke, which blinded him in one eye and impaired his brain function. The 69-year-old’s thoughts can run wild, and he can’t finish basic tasks.
He used to have a personal attendant, a service managed-care companies are cutting systemwide, The News found. But for a year and a half, he’s struggled to get help with preparing meals and cleaning his home outside Llano, where the kitchen and bathroom are filthy, and dirty laundry is piled high.
Right now, he doesn’t have a service coordinator — and says he feels abandoned. “It certainly has pushed me a hell of a lot closer to death,” Billingsley says. “I feel ashamed, living like this.”
Staff writer Jackie Wang contributed to this report.